

Pliant Therapeutics Announces Positive Long-Term Data from the INTEGRIS-IPF Phase 2a Trial Demonstrating Bexotegrast was Well Tolerated at 320 mg with Durable Improvement Shown in FVC and Across Multiple Measures
Bexotegrast was well tolerated up to 40 weeks of treatment with no drug-related serious adverse events
Combination of bexotegrast with standard of care reduced FVC decline by 80% relative to standard of care alone at Week 24
89% of bexotegrast-treated patients with an increase in FVC from baseline at Week 12 maintained an increase at Week 24
Stabilization of fibrosis as measured by QLF imaging was observed in the bexotegrast group while the placebo group showed progression of fibrosis at Weeks 12 and 24
A reduction in patient-reported cough severity was reported in the bexotegrast group in contrast to worsening in the placebo group
BEACON-IPF Phase 2b trial to be initiated in mid-2023
Company to host webcast and conference call tomorrow, Monday, May 1st at 8:00 a.m. ET
SOUTH SAN FRANCISCO, Calif., April 30, 2023 (GLOBE NEWSWIRE) -- Pliant Therapeutics, Inc. (Nasdaq: PLRX) today announced 24-week data from the 320 mg dose group of INTEGRIS-IPF, a multinational, randomized, dose-ranging, double-blind, placebo-controlled Phase 2a clinical trial of bexotegrast (PLN-74809) in patients with idiopathic pulmonary fibrosis (IPF). The 320 mg dose group met its primary and secondary endpoints demonstrating that bexotegrast was well tolerated up to 40 weeks and displayed a favorable pharmacokinetic profile. The trial's exploratory efficacy endpoints assessed changes in forced vital capacity (FVC), Quantitative Lung Fibrosis (QLF) imaging, patient reported cough severity and biomarkers. At Week 24, bexotegrast-treated patients demonstrated improvements across all of these exploratory efficacy endpoints versus placebo.
The INTEGRIS-IPF Phase 2a trial was designed to evaluate bexotegrast at once-daily doses of 40 mg, 80 mg, 160 mg or placebo for 12 weeks and 320 mg or placebo for up to 48 weeks in 119 patients with IPF.
The 320 mg group enrolled 21 patients in the active arm and 8 patients in the placebo arm. Comparable to the lower dose groups, approximately 80% of enrolled patients were on standard of care and were equally distributed between nintedanib and pirfenidone.
Bexotegrast 320 mg was Well Tolerated up to Week 40 with No Drug-Related Serious Adverse Events
The primary endpoint of the INTEGRIS-IPF trial was the evaluation of the safety and tolerability of bexotegrast. Bexotegrast was well tolerated at 320 mg up to 40 weeks of treatment with no drug-related serious adverse events (SAE) reported. Most frequently reported treatment-emergent adverse events (TEAE) were mild or moderate in severity and not related to study drug. No TEAE-related discontinuations occurred after Week 12.
The trial's secondary endpoint was an assessment of its pharmacokinetics. Bexotegrast exhibited dose-proportional increases in plasma concentrations, consistent with prior dose groups.
Bexotegrast 320 mg Group Demonstrated Treatment Effects Including Durable Improvements in FVC to Week 24
The exploratory efficacy endpoints of the INTEGRIS-IPF trial measured changes in FVC, high-resolution CT (HRCT)-based QLF, patient reported cough severity and profibrotic biomarkers to Week 24.
At Week 24, 50% of bexotegrast-treated patients experienced an increase in FVC from baseline versus 0% in the placebo group. Moreover, of the bexotegrast-treated patients who experienced an increase in FVC from baseline at Week 12, 89% maintained an increase in FVC from baseline at Week 24.
FVC Change from Baseline over 24 Weeks | FVC Change from Baseline over 24 Weeks
ITT Population | ITT Population- SoC Subgroup
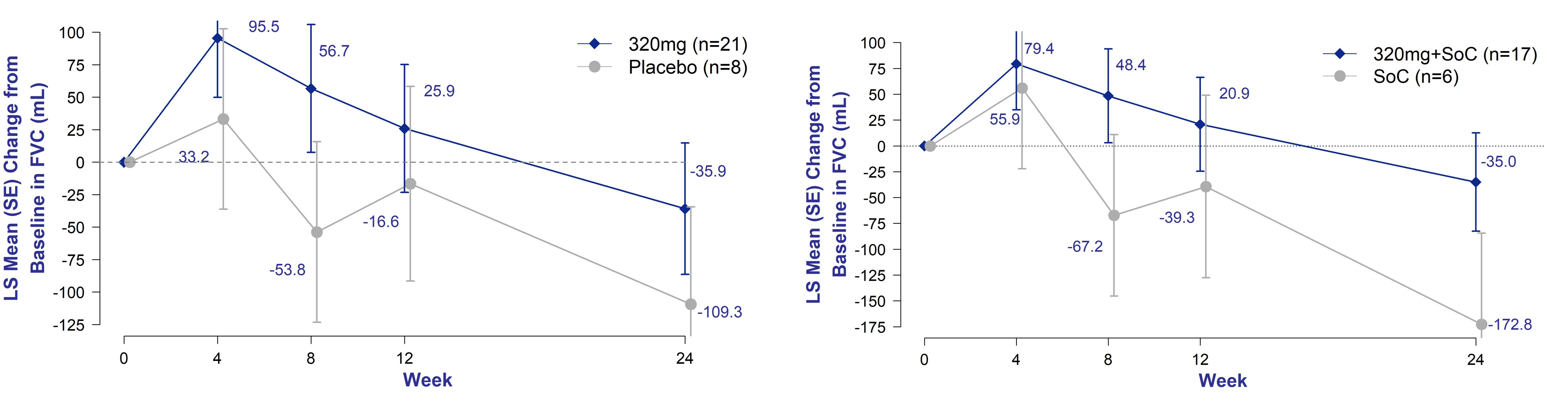
Figure 1. Change in FVC from Baseline of Bexotegrast 320 mg Over 24 Weeks
A decline of ≥10% in forced vital capacity precent predicted (FVCpp) at 12 weeks has been associated with increased mortality in IPF patients over a two-year period.1,2 At Week 24, bexotegrast-treated patients experienced a mean reduction from baseline in FVCpp of 0.8% versus a decline of 2.5% in the placebo-treated group, representing a 68% reduction in decline.
Figure 2. Proportion of Patients with FVC Change from Baseline of Bexotegrast 320 mg Over 12 and 24 Weeks versus Placebo - Intent to Treat Population
An increase in QLF score has been associated with worsening of pulmonary fibrosis.3 At Weeks 12 and 24, the mean change in QLF from baseline for bexotegrast-treated patients was below the minimally clinically important difference (MCID) of 2% while the mean change from baseline in placebo-treated patients exceeded this threshold at both timepoints.
At Week 24, bexotegrast-treated participants were more than twice as likely to show stabilization or improvement of fibrosis relative to placebo by QLF imaging.
* EU Radiology 2020 30:726-734
Figure 3. QLF Mean Percent Change from Baseline at Weeks 12 and 24 versus Placebo – Per CT Protocol Population
Chronic cough in IPF is often refractory and debilitating.4 It is an independent predictor of disease progression and may predict time to death or lung transplation.5 At Weeks 12 and 24, bexotegrast-treated patients experienced a reduction in patient reported cough severity as measured by the cough visual analog scale (VAS) versus placebo-treated patients' cough severity worsening over time.
Figure 4. Mean Change from Baseline in Cough Severity Visual Analog Scale (VAS) from Baseline Over 12 and 24 Weeks - Intent to Treat Population
Elevated integrin beta-6 plasma levels have been associated with ILD progression as defined by mortality, transplant or ≥ 10% relative reduction in FVC (mL) over 12 months.6 PRO-C3, a serum biomarker of type III collagen synthesis, is elevated in patients with IPF and associated with progressive disease.7 At Weeks 12 and 24, the bexotegrast-treated patients demonstrated a reduction in circulating biomarkers integrin beta-6 and PRO-C3 relative to placebo.
These findings support a potential antifibrotic effect of bexotegrast, consistent with its mechanism of action and preclinical findings.
"These data build on our previously reported results and highlight a favorable long-term safety profile and provide further evidence of a durable improvement in FVC, the registrational endpoint in IPF," said Éric Lefebvre, M.D., Chief Medical Officer at Pliant Therapeutics. "The INTEGRIS-IPF data provides us with confidence as we move into late-stage development. I would like to thank the patients, caregivers, investigators and clinical trial staff for their participation in the INTEGRIS-IPF study. We are excited to now turn our attention to initiating BEACON-IPF, our Phase 2b 52-week trial in patients with IPF, in mid-2023."
"These data demonstrate a consistent signal across physiologic, radiographic and symptomatic treatment effects of bexotegrast, along with a favorable tolerability profile," said Lisa H. Lancaster, M.D., Professor of Medicine, Vanderbilt University Medical Center and INTEGRIS-IPF Principal Investigator. "I am encouraged by the evidence of bexotegrast's favorable impact on cough severity, a debilitating symptom in IPF patients."
Bexotegrast Clinical Development Next Steps
Pliant is planning to initiate BEACON-IPF, a 52-week, multinational, randomized, placebo-controlled Phase 2b clinical trial of bexotegrast at doses of 160 mg and 320 mg in approximately 270 patients with IPF, in mid-2023.
INTEGRIS-IPF Multinational Phase 2 Trial of PLN-74809 (NCT04396756)
INTEGRIS-IPF was a Phase 2a, multinational, randomized, dose-ranging, double-blind, placebo-controlled trial evaluating the safety, tolerability, and pharmacokinetics of PLN-74809 administered in patients with IPF. Patients were enrolled in doses of 40 mg, 80 mg, 160 mg or 320 mg with a 3:1 randomization ratio (active:placebo) and stratification based on use of standard of care therapy. The primary endpoint was the evaluation of PLN-74809 safety and tolerability and the secondary endpoint was the assessment of pharmacokinetics across a dose range. Exploratory endpoints measured change in Forced Vital Capacity (FVC), HRCT-based Quantitative Lung Fibrosis (QLF) score and selected biomarkers.
Background on Idiopathic Pulmonary Fibrosis
IPF is a chronic, progressive, fibrosing lung disease of unknown cause with few treatment options and a poor prognosis. Patients experience debilitating symptoms, including shortness of breath and difficulty performing daily activities, such as walking and talking. Currently, there is no pharmacological cure for IPF, with neither of the approved two therapies demonstrating an ability to stop the progression of IPF. Therefore, there is a high unmet need for new therapeutic options to address the symptoms and modify the disease progression of this grievous illness.
Conference Call and Webcast Information
The Company will host a conference call and webcast with a slide presentation tomorrow, Monday, May 1, 2023 at 8:00 a.m. ET to discuss this update. Members of Pliant management will be joined by Dr. Toby Maher, a Professor of Medicine and Director of Interstitial Lung Disease at Keck School of Medicine, University of Southern California, Los Angeles. Interested parties may access the webcast live via Pliant's website at https://edge.media-server.com/mmc/p/ney8cvgr. The live audio of the conference call can be accessed by telephone by registering in advance at the following link: Pliant Therapeutics INTEGRIS-IPF Conference Call. Upon registration, all telephone participants will receive the dial-in number along with a unique passcode to access the call. An archived replay of the webcast via Pliant's website for 30 days following completion of the event.
Forward-Looking Statements
Statements contained in this press release regarding matters that are not historical facts are "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995. Words such as "may," "will," "expect," "anticipate," "estimate," "intend," and similar expressions (as well as other words or expressions referencing future events, conditions, or circumstances) are intended to identify forward-looking statements. These statements include those regarding future development of bexotegrast in PSC, including plans to initiate a Phase 2b clinical trial of bexotegrast in mid-2023; and statements regarding the safety, tolerability, pharmacodynamics and therapeutic potential of bexotegrast. Because such statements deal with future events and are based on our current expectations, they are subject to various risks and uncertainties and actual results, performance or achievements of Pliant Therapeutics could differ materially from those described in or implied by the statements in this press release. These forward-looking statements are subject to risks and uncertainties, including those related to the development and commercialization of our product candidates, including any delays in our ongoing or planned preclinical or clinical trials, the impact of the ongoing COVID-19 pandemic on our business, operations, clinical supply and plans, our reliance on third parties for critical aspects of our development operations, the risks inherent in the drug development process, the risks regarding the accuracy of our estimates of expenses and timing of development, our capital requirements and the need for additional financing, and our ability to obtain and maintain intellectual property protection for our product candidates. These and additional risks are discussed in the sections titled "Risk Factors" and "Management's Discussion and Analysis of Financial Condition and Results of Operations" in our Annual Report on Form 10-K for the year ended December 31, 2022 which is available on the SEC's website at www.sec.gov. Unless otherwise noted, Pliant is providing this information as of the date of this news release and does not undertake any obligation to update any forward-looking statements contained in this document as a result of new information, future events or otherwise.
About Pliant Therapeutics, Inc.
Pliant Therapeutics is a clinical stage biopharmaceutical company focused on discovering and developing novel therapies for the treatment of fibrosis. Pliant's lead product candidate, bexotegrast (PLN-74809), is an oral small molecule dual selective inhibitor of αvß6 and αvß1 integrins that is in development in the lead indications for the treatment of idiopathic pulmonary fibrosis, or IPF, and primary sclerosing cholangitis, or PSC. Bexotegrast has received Fast Track Designation and Orphan Drug Designation from the U.S. Food and Drug Administration (FDA) in IPF and PSC and Orphan Drug Designation from the European Medicines Agency in IPF and PSC. Pliant is currently conducting Phase 2a trials of bexotegrast in the lead indications of IPF and PSC. Pliant has also developed PLN-1474, a small molecule, selective inhibitor of αvß1 for the treatment of nonalcoholic steatohepatitis, or NASH with liver fibrosis. Pliant is initiating a Phase 1 study for its third clinical program, PLN-101095, a small molecule, dual-selective inhibitor of αvß8 and αvß1 integrins, that is being developed for the treatment of solid tumors. In addition to clinical stage programs, Pliant currently has a preclinical program targeting muscular dystrophies. For additional information about Pliant Therapeutics, visit www.PliantRx.com and follow us on Twitter, LinkedIn, Facebook and YouTube.
Investor and Media Contact:
Christopher Keenan
Vice President, Investor Relations and Corporate Communications
Pliant Therapeutics, Inc.
ir@pliantrx.com
1 Paterniti MO et al. Ann Am Thorac Soc. 2017 Sep 14(9):1395-1402.
2 Khan FA et al. Am J Respir Crit Care Med. 2022 Apr 15;205(8):936-948.
3 Kim GHJ et al. Ther Adv Respir Dis. 2021 Jan (15): 1–11.
4 van Manen MJG et al. Eur Respir Rev 2016; 25: 278–286.
5 Ryerson CJ et al. Respirology 2011; 16: 969–975.
6 Organ LA et al. Respir Res. 2019 Jul 12;20(1):148.
7 Bowman WS et al. Lancet Respir Med. 2022 Jun;10(6):593-602.
Photos accompanying this announcement are available at
https://www.globenewswire.com/NewsRoom/AttachmentNg/00768312-f9ac-422c-8206-f0879d8958dd
https://www.globenewswire.com/NewsRoom/AttachmentNg/742e2d1e-8226-46f7-ae66-e9bed71ee1a9
https://www.globenewswire.com/NewsRoom/AttachmentNg/897ba34b-b2d9-4a56-992f-6b706ad1cc9c
https://www.globenewswire.com/NewsRoom/AttachmentNg/09ec2006-7ca8-431a-b8b0-3e4e8584039b
